Porto-sinusoidal vascular disease (PSVD)
Structural Liver Disease
Description
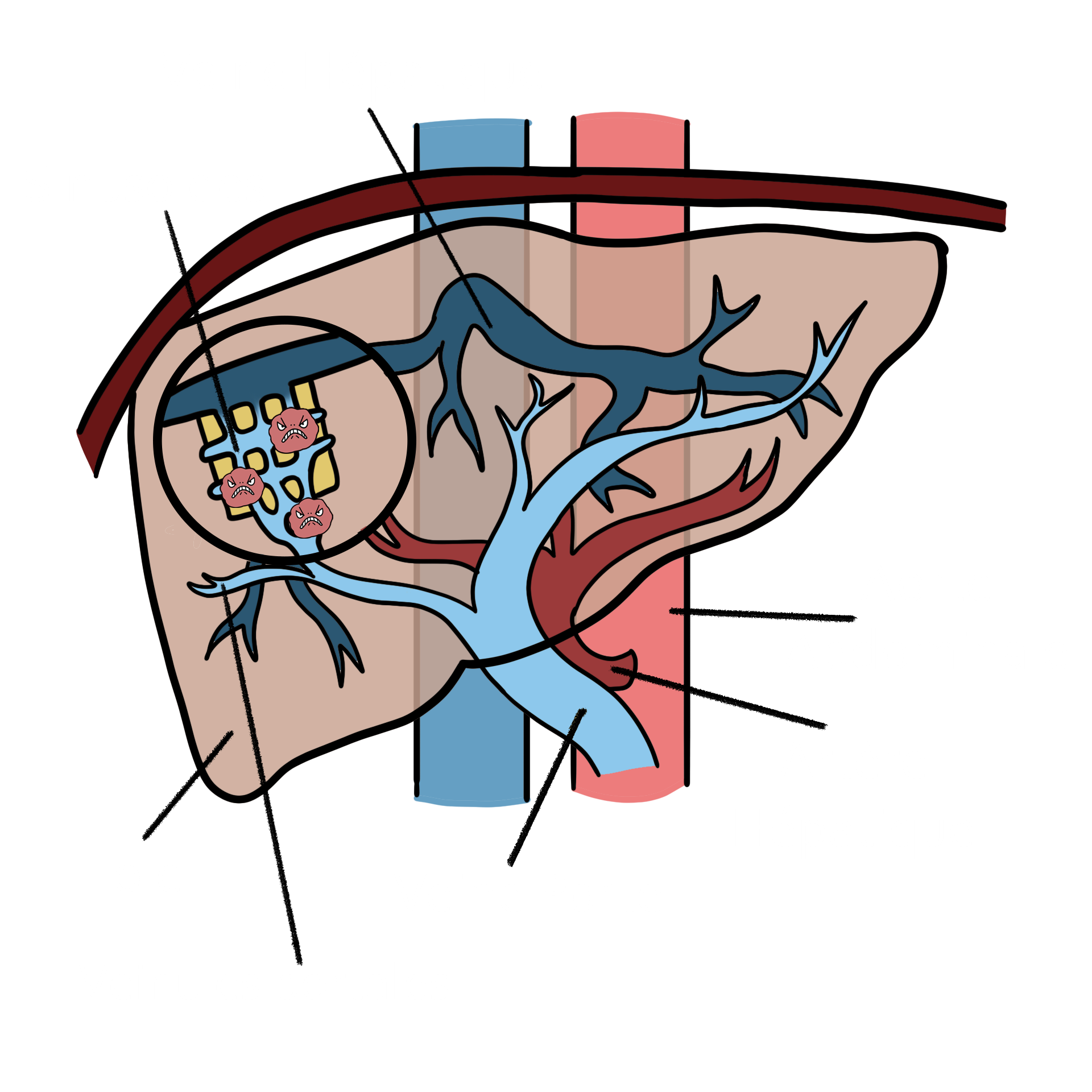
Porto-sinusoidal vascular disorder, previsously mentioned as idiopathic portal hypertension or non-cirrhotic portal hypertension, is a heterogeneous condition evolving the small vessels in the liver, namely small portal venules and/or sinusoids, usually recognized when signs related to portal hypertension (increased presion in abdominal vessels) arise.
What are the symptoms?
As there is a wide spectrum of clinical presentation, symptoms are varied and nonspecific:
- No symptoms
- Fatigue
- Gastrointestinal bleeding
- Accumulation of fluids in the abdomen (ascites)
- Leg oedema/swelling
- Confusion (hepatic encephalopathy)
When is PSVD suspected?
Different scenarios may be present:
- Unexplained liver profile blood analyses with or without signs of portal hypertension (enlarged spleen, oesophageal varices, low platelets, upper gastrointestinal hemorrhage, ascites, confusion…) in the absence of cirrhosis;
- Disagreement between portal hypertension severity and normal or almost normal liver profile blood analyses;
- Portal hypertension signs (enlarged spleen, oesophageal varices, thrombopenia) the presence of a low elastography (<10Kpa) as documented in a Fibroscan® exam.
Diagnosis
PSVD is estimated to be underdiagnosed as it may be mistaken with liver cirrhosis. In order to establish the diagnosis in the presence of a suspected PSVD, a good and representative liver biopsy must be done.
The final diagnosis is made when no signs of liver cirrhosis are found in the liver biopsy together with the presence of a specific lesion of PSVD (obliterative portal venopathy, nodular regenerative hyperplasia or incomplete septal fibrosis) or one specific sign of portal hypertension (gastric and/or esophageal varices, hypertensive upper digestive hemorrhage or portosystemic collaterals found in CTscan or MRI). Patients without liver cirrhosis in liver biopsy and with other non-specific signs of portal hypertension and non-specific findings of PSVD histology may also be diagnosed with this disease.
What are the causes?
Porto-sinusoidal vascular disorder is related with several risk factors that may lead to vascular damage inside the liver. Blood diseases (for example a myeloproliferative disorder), prothrombotic conditions (genetic or acquired), immunological disorders (notably common variable immune deficiency, autoimmune hepatitis, HIV infection, etc.), exposure to drugs commonly used in chemotherapy like oxaliplatin, or in immunosuppression like azathioprine, or in HIV treatment like didanosine have been implicated, as well as other genetic diseases or repeated gastrointestinal or urinary tract infections. Autoimmunity and downregulation of some genes associated to vascular homeostasis have been recently found to be related to PSVD.
Management
Patients with PSVD without portal hypertension must be followed in order to evaluate progression of the disease.
Patients with PSVD and portal hypertension are managed almost like a patient with liver cirrhosis. Non-invasive methods used to esophageal varices screening, like the simultaneous use of platelet count and liver elastography are not applied to PSVD patients, reason why in the presence of portal hypertension signs all patients must perform an upper endocopy.
As patients with PSVD are more prone to develop portal vein thrombosis (development of a blood clot inbeneath the portal vein – the vein that lead the blood from the intestins towards the liver), a Doppler ultrasound should be performed every 6-months.
Patients with complications related to portal hypertension that do not respond to medical or endoscopic treatment should be considered for TIPS - Transjugular intrahepatic portosystemic shunt. This is a radiologic procedure in which a stent (a tubular device) is placed in the middle of the liver to reroute the blood flow ir order to decrease portal hypertension and related complications.
Indications for liver transplantation in patients with PSVD are the same for liver cirrhosis (complications realted to portal hypertension that do not respond to standard treatments and/ or progression to liver failure), with good outcomes.
Portal vein thrombosis
Portal vein thrombosis is a frequent finding in patients with PSVD and portal hypertension, in up to 13-45% of patients. A prothrombotic condition is found in 1/5 of the patients. Anticoagulation must be started in order to avoid progression. The choice of anticoagulation depends on related precipitant to portal vein thrombosis development, the degree of liver failure and coexistence and degree of renal insufficiency.
Who is affected?
PSVD is a rare vascular liver disease, affecting both women and men, in proportions that depend on the geographical area and predisposing risk factor. PSVD is commonly diagnosed in the 4th-5th decades of life.
What can I do?
Medication:
Follow and understand medical prescriptions and inform others of these prescriptions (i.e. with a card in your wallet). Medication currently used in PSVD with portal hypertension can contemplate non-selective beta-blockers to lower the pressure in the portal venous circulation, to avoid bleeding from varices; diuretics in order to control intraabdominal fluid (ascites) production; therapy directed towards control of hepatic encephalopathy, as laxatives, rifaximin and zinc; anticoagulation in the setting of portal vein thrombosis.
Diet:
Avoid alcohol or any co-factor for liver disease, in particular overweight. Therefore a balanced diet (green Mediterranean diet) is recommended.
Family planning:
Pregnancy should be anticipated, prepared and followed by a multidisciplinary team.
Do my family and I need to get genetically tested?
No. PSVD is not a congenital disease and, till date, no gene has been directly implicated in its genesis. Nevertheless, you may have some tests performed on DNA screening for congenital causes of PSVD.
Do I need medical checkups?
Yes, it is very important to have regular blood tests, imaging (with Doppler study) and outpatient clinic checkups, at least every 6 months regularly.
How can I find a specialist?
PSVD may need to be managed by a doctor or a hospital network with experience or an interest in PSVD. PSVD is a rare disease that not every doctor has an interest in or experience with. However, some hospitals are part of the Europe-wide reference network for rare liver diseases, ERN RARE-LIVER. This means that patients seen at hospitals within the network can benefit from the expertise of specialists who work at other hospitals within the network. For more information about the ERN RARE-LIVER, visit https://rare-liver.eu/. You can find information and patient support in the section “patients” on the ERN RARE-LIVER website (https://rare-liver.eu/).
Disclaimer
The information provided free of charge on our website has been compiled to the best of our knowledge in order to give interested readers an initial overview of possible diseases and treatment options. They are intended solely for informational purposes and in no case replace personal advice, examination or diagnosis by authorized doctors.